Primary care physicians are facing a burden to regulate access to specialty care for patients with opioid use disorder (OUD).
Not unlike the prior authorization process, where a patient’s primary care physician (PCP) is expected to complete a form to “approve” patient access to a specialist or speciality treatment, the DEA is proposing a rollback on telehealth services that requires PCPs to become gatekeepers to care.
The ruling would require patients with OUD to visit a physician in-person to receive ongoing buprenorphine prescriptions, often forcing patients to go through their PCP to do so. The proposal is currently under review until November, but the thought of adding more to physicians’ overloaded plates is worth examining, as it adds undue strain to our already-inadequate OUD treatment infrastructure.

For time sensitive treatment, telehealth is immensely effective
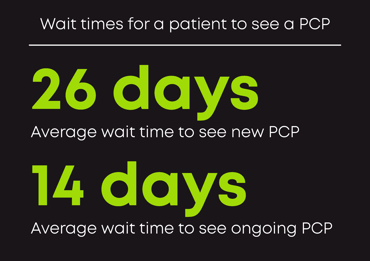 As a primary point of contact, PCPs already have a slew of responsibilities to consider. Busy schedules mean patients are waiting 26 days for an appointment with a new provider. For those who already have a regular PCP, 60% of patients wait two weeks and only 10% are able to access care the same day. Not to mention PCP shortages have grown following the COVID-19 pandemic. If everyone seeking care was able to access it, we would need 180,400 physicians to fill the deficit.
As a primary point of contact, PCPs already have a slew of responsibilities to consider. Busy schedules mean patients are waiting 26 days for an appointment with a new provider. For those who already have a regular PCP, 60% of patients wait two weeks and only 10% are able to access care the same day. Not to mention PCP shortages have grown following the COVID-19 pandemic. If everyone seeking care was able to access it, we would need 180,400 physicians to fill the deficit.
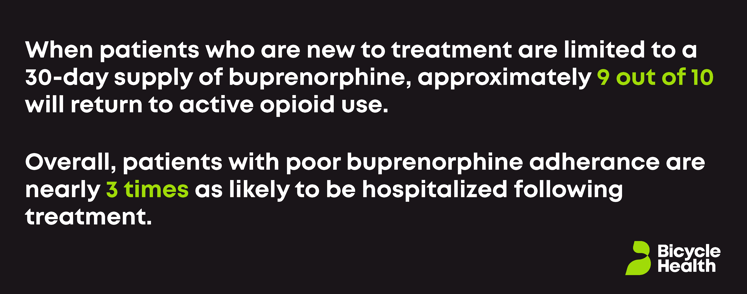
Patients and providers need a system that supports regularly accessible treatment. The potential DEA ruling would make quality care even harder to access—and to provide—by further restricting access behind a referral and prior authorization barrier. Additionally, required in-person evaluations after a 30-day supply of buprenorphine puts patients at a higher risk of falling off their treatment plan, which could result in relapse and even death. When patients who are new to treatment are limited to a 30-day supply of buprenorphine, approximately 9 out of 10 will return to active opioid use, according to a 2011 study. Overall, patients with poor buprenorphine adherence are nearly 3 times as likely to be hospitalized following treatment.
Conversely, we know treatment of OUD via telehealth is not only easier to access (taking the burden off of in-person providers), it is also effective in treating a larger subset of people at a faster rate. Given the dismal statistics related to OUD, the more programs and providers that deliver above-average outcomes, the better.
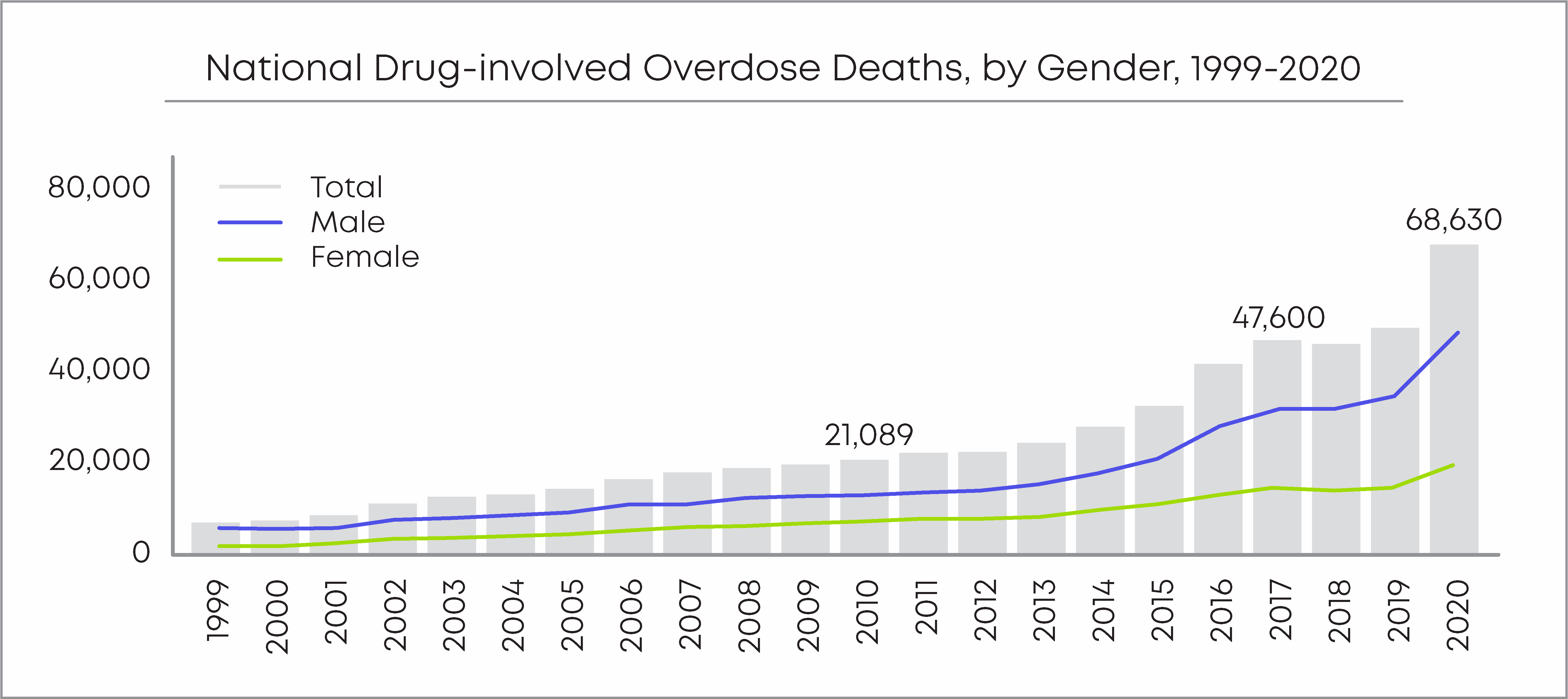
“The increasingly alarming mortality risk [of OUD], it is critical to consider the accessibility of evidence-based treatment especially relative to that of the unpredictable, illicitly manufactured opioids that are driving overdose fatalities,” Tamara Beetham, MPH, recently said in reference to a study she authored on the positive effects of telehealth for people with OUD during the pandemic. “Having a telehealth option may help alleviate barriers to life-saving care.”
Put another way, and as said at a recent FDA Foundation symposium, “When it’s easier to get illicit fentanyl than it is to get buprenorphine, we’re doing something very wrong.”
The DEA is ignoring the impact of tele-OUD treatment
It’s clear from the proposed rule that the DEA has no intention of improving access to medications used to treat OUD. In-person appointments with a PCP might work for some, but for many patients and providers, telehealth treatment is the best option. There is no medical advantage to requiring in-person visits with a DEA-registered health care provider. There is no reason to believe that in-person care is better or safer than OUD care provided via telehealth. In fact, telehealth treatment is seemingly more effective than in-person; there is strong evidence from CDC, CMS, and NIDA researchers to indicate that telehealth has improved retention for medication for opioid use disorder (MOUD) programs. Even providers agree that telehealth treatment can lessen physician burden and allow them to provide live-saving care to more patients.
The DEA’s proposed rule is inconsistent with the idea that people suffering from OUD deserve treatment. Tele-OUD care is not only safe, it’s effective. Patient care should be the priority and that extends to people with OUD. In-person contact is unnecessary for both diagnosis or prescription.
“Either the DEA misunderstands the value of direct physical contact in treating OUD,” Bicycle Health board member Patrick Kennedy recently wrote, “or perhaps the unstated goal is to limit buprenorphine access through yet another unnecessary barrier.”
At Bicycle Health, we believe that successful treatment can come in many forms: not just from PCPs, but also from specialists in addiction treatment—providers who have dedicated the time and effort to become experts. They have the knowledge, expertise, and time to offer patients the care and attention they not only deserve, but need. Patients deserve a treatment plan that works for them, one that doesn’t over burden a subset of providers. We must expand access to care to reach as many people as possible.